As an endodontist, I regularly see patients who come in convinced they need a root canal, only to discover the culprit is dentin hypersensitivity. And occasionally, the reverse is true — someone brushing off their “cold sensitivity” for months turns out to have a cracked tooth that absolutely requires intervention. The difference between these two scenarios isn’t always obvious from the outside, but understanding the science behind why teeth hurt is the first step toward the right solution.
Today, I’ll go beyond the standard advice and walk you through what’s actually happening inside your tooth when it zings — and more importantly, how to tell when it’s something you can manage at home versus when it’s time to call your dentist.

The Science of Sensitivity: What’s Actually Happening Inside Your Tooth
Before talking about causes and treatments, it’s worth understanding the mechanism — because it’s genuinely fascinating, and it shapes every treatment decision we make.
Your tooth isn’t solid. Beneath the hard outer enamel lies dentin, a living tissue riddled with thousands of microscopic channels called dentinal tubules. These tubules run from the outer surface of the tooth all the way inward to the nerve-rich pulp, and they’re filled with fluid.
When dentinal tubules are exposed at the surface, external stimuli cause changes in fluid flow within them. This shift in fluid movement stimulates the myelinated nerve fibers located in the pulp, producing the characteristic sharp, transient pain of dentin hypersensitivity. Wikipedia This is known as Brännström’s Hydrodynamic Theory — first proposed in the 1960s, and still the most widely accepted explanation for tooth sensitivity today.
Cold thermal stimuli cause the dentinal fluid to contract, creating an outward shift in flow that activates the mechanical receptors at the pulpal end of the tubules. The coefficient of thermal expansion of tubule fluid is roughly ten times that of the tubule wall itself, which is why temperature changes produce such a pronounced response. Dentalcare
Here’s the key clinical implication: the more open and numerous the exposed tubules, the more intense the sensitivity. Research using scanning electron microscopy has shown that the number of tubules in sensitive dentin is approximately eight times greater than in non-sensitive dentin, and the tubules in sensitive areas are also wider. PubMed Central This is why simply covering or blocking those tubules — whether with a desensitizing toothpaste or a professional bonding agent — forms the logical backbone of most treatments.
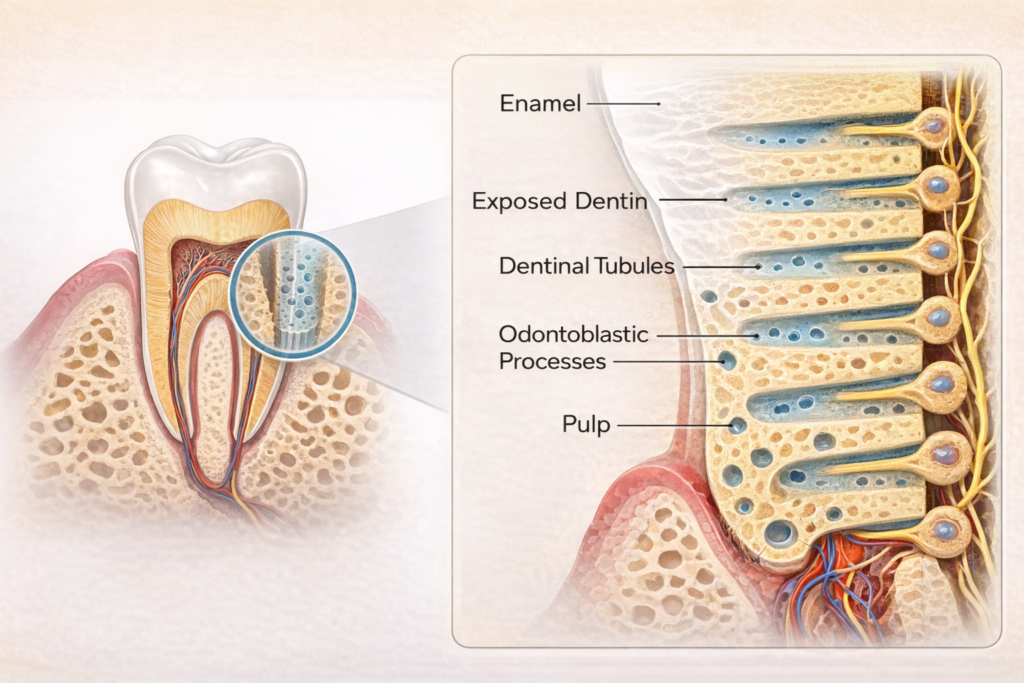
Figure 1. Schematic diagram of exposed dentin and dentinal tubules
Why Are Your Tubules Exposed? The 3 Main Causes
1. Non-Carious Cervical Lesions (NCCL)
This is the most common cause of tooth sensitivity. It involves a V-shaped or dish-shaped notch forming at the junction of the tooth and gum — a loss of hard tooth tissue that occurs without any cavities. NCCL is not caused by a single factor, but by a combination of erosion, abrasion, and occlusal stress (abfraction) acting together. PubMed

The most common contributing factors include:
- Aggressive Brushing: Using a horizontal “scrubbing” motion wears away the thinnest point of enamel at the tooth’s cervical region. Excessive horizontal brushing and frequent consumption of acidic foods and beverages are well-documented risk factors for cervical tooth wear. Wiley Online Library
- Bruxism (Teeth Grinding/Clenching): Repetitive occlusal stress can induce micro-fractures in the cervical enamel, PubMed Central causing the tooth’s most vulnerable “waist” region to progressively chip and flake away.
- Hard or Tough Foods: Regularly chewing hard foods concentrates occlusal load on the cervical area, accelerating wear over time.
- Acidic diet: Frequent exposure to acidic drinks softens the enamel surface, making it far more susceptible to being worn away by brushing. This combination of erosion followed by abrasion is a particularly fast route to dentin exposure.
The prevalence of NCCL varies widely across studies — from 10% to over 90% — and increases with age, most commonly affecting the buccal surface of maxillary premolars. PubMed Since the cervical region is where enamel is at its thinnest, even minor wear quickly exposes the underlying dentin, triggering sensitivity.
2. Gingival Recession (Receding Gums)
When the gums pull back, the tooth root becomes exposed. Unlike the crown, the root has no enamel — only a thin layer of cementum that wears away quickly, leaving the underlying dentin (and its open tubules) directly exposed to the oral environment. Because lost gum tissue and supporting bone do not regenerate on their own, the goal of treatment shifts entirely to halting further recession and protecting the exposed root surface.

3. Cracked Tooth Syndrome — The One You Don’t Want to Miss
This is where my perspective as an endodontist becomes especially relevant. According to the American Association of Endodontists (AAE), poor occlusion, bruxism and parafunctional habits, and repetitive wedging forces are all potential causes of tooth cracks — and when left untreated, cracks can allow bacteria and biofilms to progress toward the pulp, resulting in pulp necrosis. American Association of Endodontists
A cracked tooth can feel identical to ordinary dentin hypersensitivity, which is exactly what makes it dangerous to self-diagnose.

Is It Sensitivity — Or Is It a Crack? How to Tell the Difference
This is perhaps the most clinically important question in this article. Dentin hypersensitivity always occurs in response to an external stimulus — it is rarely, if ever, continuous or spontaneous. If a patient reports pain that lingers, occurs without provocation, or is not clearly tied to a specific trigger, diagnoses other than simple dentin hypersensitivity must be considered. PubMed Central
Here’s a practical way to think about it:
| Feature | Dentin Hypersensitivity | Cracked Tooth / Pulpitis |
|---|---|---|
| Onset | Triggered by stimulus (cold, air, sweet) | Can be spontaneous or triggered |
| Duration | Sharp but brief — disappears when stimulus is removed | Lingers 30+ seconds after stimulus is gone |
| Biting pain | Rarely | Often — especially on release of biting pressure |
| Location | Often multiple teeth, cervical area | Usually one specific tooth |
| Night pain | Uncommon | Common with irreversible pulpitis |
According to AAE diagnostic guidelines, symptomatic irreversible pulpitis — the stage at which a root canal becomes necessary — is characterized by sharp pain upon thermal stimulus with lingering pain often lasting 30 seconds or longer after the stimulus is removed, spontaneous or unprovoked pain, and pain that may be worsened by lying down or bending over. American Association of Endodontists
If your “cold sensitivity” doesn’t go away within a few seconds, see your dentist. Don’t wait.
Home Care: What Works and Why
Desensitizing Toothpaste
The first line of defense for most patients. Products containing Potassium Nitrate (KNO₃) work by a fundamentally different mechanism than toothpastes that occlude the tubules. Potassium ions diffuse along the dentinal tubules and depolarize the nerve cells, making them less responsive to excitatory stimuli — though the effect is cumulative and may take several weeks of consistent use to become noticeable. PubMed Central
More recent formulations containing nano-hydroxyapatite, arginine, or calcium sodium phosphosilicate (bioglass) work through a complementary approach: physically depositing mineral particles into the open tubule openings to restrict fluid movement. For patients with moderate sensitivity, combining both mechanisms — nerve-blocking and tubule-occluding — often yields better results.
Keep in mind that no toothpaste addresses the underlying structural cause. If you’re relying on desensitizing toothpaste indefinitely without getting a diagnosis, you may be masking a condition that’s quietly progressing.
Correcting Your Brushing Technique
Switch from a horizontal scrubbing motion to the Roll Technique — placing the bristles at a 45-degree angle to the gum line and rolling gently toward the tooth. Use a soft-bristled brush and let the bristles do the work, not your wrist. This single habit change can substantially slow the progression of cervical wear.
Professional Treatments: A Step-by-Step Guide
If home care isn’t enough, professional intervention is necessary based on the severity of your symptoms.
Step 1 — In-Office Desensitization
For mild cases, your dentist applies high-concentration agents directly to the exposed dentin surface. The most commonly used agents are:
Glutaraldehyde/HEMA-based agents (e.g., Gluma): Cause protein precipitation within the tubules, effectively plugging them and reducing fluid movement. Clinical studies show rapid reduction in sensitivity following application.
Fluoride Varnish: Creates a calcium fluoride layer over the exposed tubules, providing both a physical seal and ongoing remineralization of the dentin surface.

The procedure is quick and painless, but the protective layer can be dissolved by acidic foods, saliva, and friction over time — meaning re-application may be needed.
Step 2 — Cervical Restoration (Fillings)
When there is visible notching or wear at the cervical area, a restoration is the most durable solution. Composite resin has demonstrated strong clinical performance in cervical restorations and is generally the recommended material of choice, PubMed Central though material selection depends on the specific clinical situation:
- Glass Ionomer (GI): Releases fluoride continuously, which helps protect the surrounding tooth structure and may slow further progression. Best suited for root-surface lesions where moisture control is challenging.
- Composite Resin: Superior in strength and aesthetics, and bonds directly to dentin through modern adhesive systems, creating a physical barrier over the exposed tubules. The material of choice for visible anterior and premolar areas.

Step 3 — Root Canal Therapy & Crowns
When sensitivity has crossed the line into irreversible pulpitis — or when a crack has extended deep enough to reach the nerve — root canal therapy is necessary to eliminate the source of pain. Following the procedure, a full-coverage crown is placed to protect the tooth from further fracturing. According to the AAE, untreated cracks allow bacteria to progress toward the pulp, and without intervention, can lead to pulp necrosis and complete tooth loss. American Association of Endodontists The earlier a crack is caught, the more treatment options remain available.
A Comparison Table: Home Care vs. Professional Treatment
| Approach | Best For | Limitations |
|---|---|---|
| Desensitizing Toothpaste | Mild, diffuse sensitivity | Symptomatic relief only; doesn’t fix the cause |
| Correct Brushing | Preventing further wear | No effect on existing damage |
| In-Office Desensitization | Moderate sensitivity, early NCCL | Temporary; may need repeat applications |
| GI / Resin Restoration | Visible cervical notching | Requires clinical diagnosis; varies by depth |
| Root Canal + Crown | Irreversible pulpitis, cracked tooth | Necessary when nerve is involved |
Final Thoughts
Tooth sensitivity is one of those conditions where the symptom — a brief, sharp zing — rarely matches the seriousness of what might be causing it. A simple exposed tubule and a cracked tooth heading toward nerve damage can feel almost identical from the patient’s perspective. That’s why the most important thing you can do isn’t switching toothpaste — it’s getting an accurate diagnosis.
If you’re experiencing persistent sensitivity, consult your dentist to find the right solution for your smile. Early intervention is the best way to avoid more complex procedures down the line — and that “zing” you feel today might be the last warning your tooth is able to give.
“Stop the Zap: An Endodontist’s Guide to Tooth Sensitivity — What’s Really Happening Inside Your Tooth”에 대한 2개의 생각