From the Endodontist’s Perspective
As a specialist in endodontics and conservative dentistry, my primary goal is always to preserve the natural tooth whenever possible. Root canal treatment (RCT) has a high overall success rate, but the complexity of root canal anatomy — with its maze of lateral canals, isthmuses, and accessory foramina — means that a percentage of cases will develop persistent periapical pathology despite treatment.
When that happens, extraction is not the only answer. This post walks through the clinical decision-making process I use when a patient presents with a failing root canal, using a real case from my practice as a reference point.
Three Options When Root Canal Treatment Fails
Not every failed root canal ends in extraction. Clinically, there are three pathways, and the right choice depends on individual anatomy, restoration status, and the patient’s own goals.
| Nonsurgical Retreatment | Apicoectomy (Surgery) | |
|---|---|---|
| Approach | Through the crown, no incision | Surgical flap, direct access to apex |
| Best for | Coronal leakage, missed canals, inadequate fill | Persistent lesion after retreatment, calcified canals, post/crown present |
| Anesthesia | Local (chair-side) | Local (minor surgery) |
| Recovery | Minimal | 3–5 days swelling/bruising |
| Success rate | ~75–85% | ~84–91% (microscopic technique) |
| Tooth structure loss | Low | Root shortened by ~3mm |
| When NOT suitable | Calcified canal, large post, crown | Vertical root fracture, poor perio support |
Option 3 — Extraction becomes necessary when neither of the above is feasible: in cases of vertical root fracture, severe bone loss, or when the tooth simply cannot be restored to function. In such cases, an implant or bridge is discussed as the next step.
A Patient’s Story: “My Gum Has Been Swollen for Weeks”
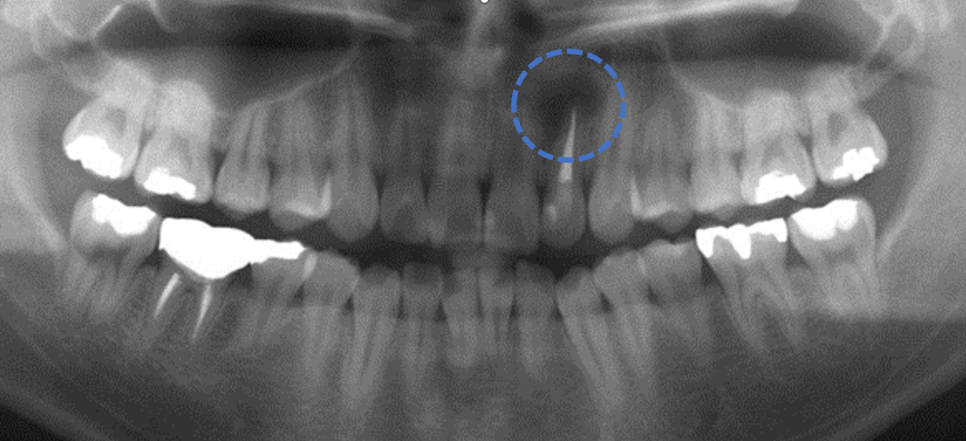
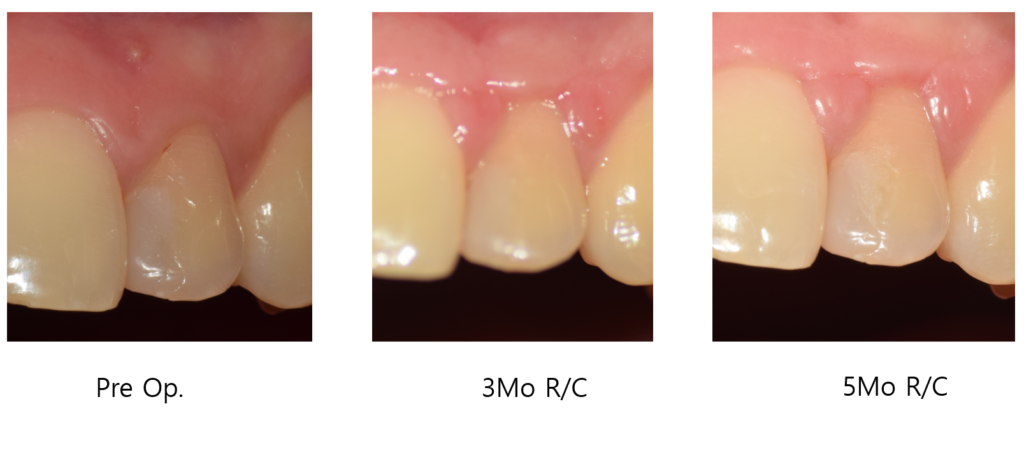
A 29-year-old male patient came to my clinic with a chief complaint of recurring gum swelling and spontaneous discharge near his upper left lateral incisor (#22). He reported that the area had been intermittently swollen for the past several weeks, and that a small pimple-like bump(Parulis) on the gum — a sinus tract — would occasionally drain on its own, providing temporary relief before returning.
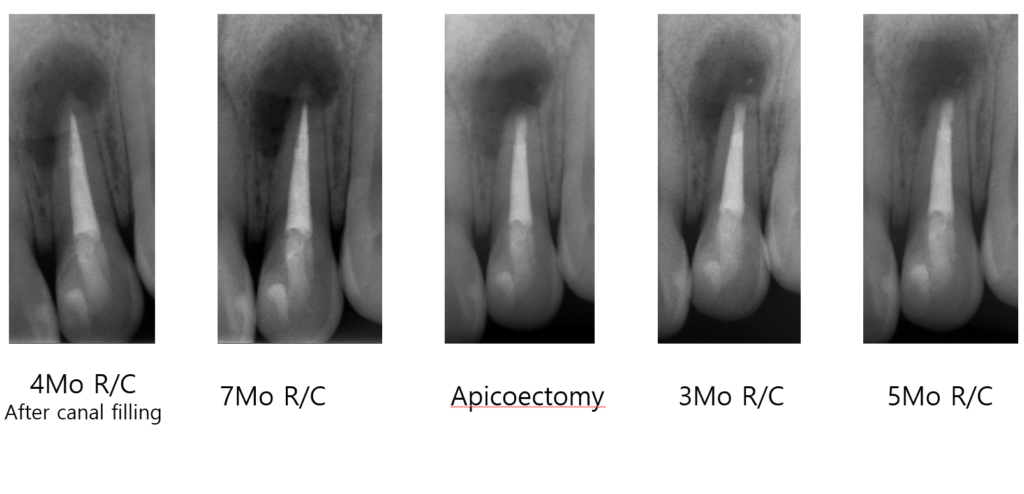
He mentioned the tooth had been root-canal-treated approximately 10 years ago, and that he had undergone nonsurgical retreatment at another clinic roughly 7 months prior — but the swelling never fully resolved.
On radiographic examination, a large periapical radiolucency was clearly visible at the root apex, consistent with chronic apical periodontitis. GP cone tracing through the sinus tract confirmed the source of infection.
Why We Chose Apicoectomy — and How It Was Done
In this patient’s case, nonsurgical retreatment had already been attempted. After 7 months of follow-up with no radiographic improvement, the decision was made to proceed with microscopic apicoectomy. The patient was strongly motivated to keep his natural tooth, and the root anatomy was favorable.
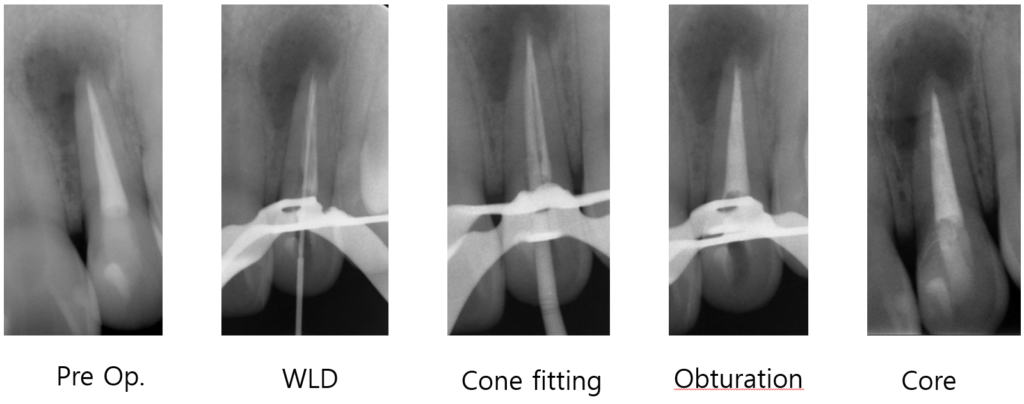
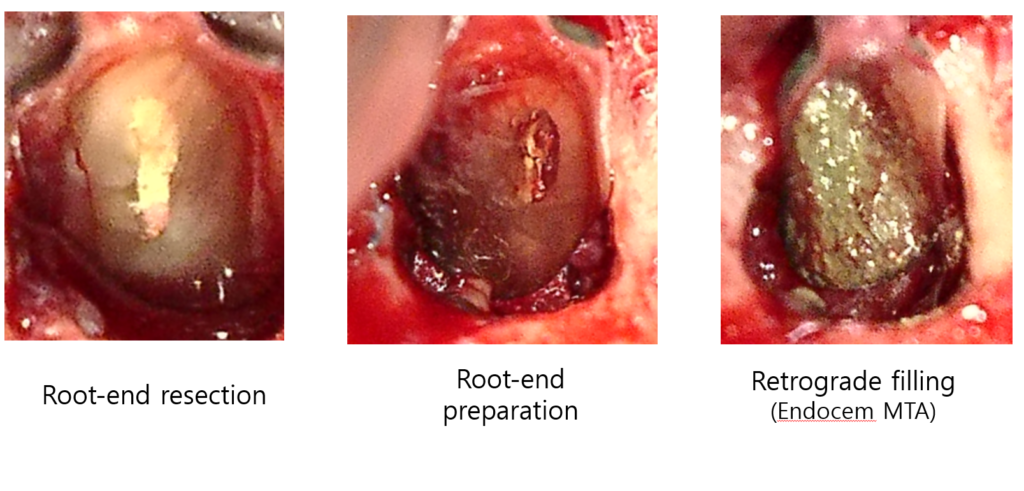
Surgical steps:
1. Papilla-based incision — A precision incision designed to preserve the interdental papilla, minimizing the risk of gingival recession in the esthetic zone. For anterior teeth, this detail matters significantly for the long-term cosmetic outcome.
2. Root-end resection (3mm) — The apical 3mm of the root was resected at a near-zero bevel angle. This region harbors the highest concentration of lateral canals and bacterial biofilm — the primary reason retreatment alone often fails.
3. Methylene blue staining under microscope — Under high magnification, the resected surface was stained to screen for microcracks and accessory canals that would otherwise be invisible to the naked eye. This step is only possible with a surgical microscope, and it fundamentally changes the diagnostic accuracy of the procedure.
4. Retrograde preparation and MTA backfill — Using ultrasonic tips, a 3mm cavity was prepared in the root end and filled with Endocem MTA(Bioceramic materials) — a bioceramic material with excellent sealing ability, biocompatibility, and performance even in a moist environment
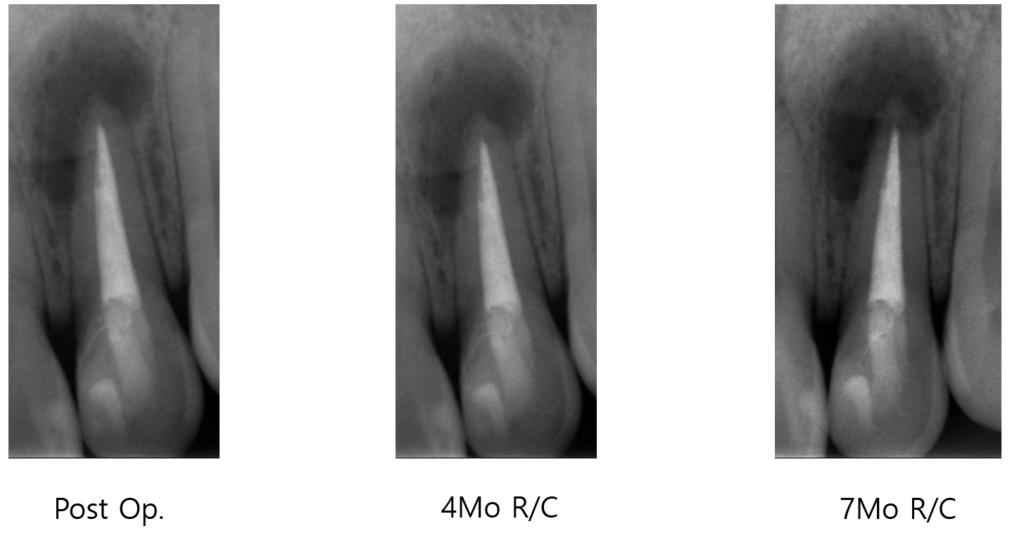
Treatment Outcomes: 5 Months, and Beyond
At the 5-month follow-up, the sinus tract had completely resolved — no more swelling, no discharge. Periapical radiographs showed clear bone regeneration beginning to fill in the previously dark lesion area.
To put tis in context with published evidence:
- A 2019 study reported that 91.4% of teeth showed successful clinical and radiographic healing at the 1-year mark following apicoectomy with retrograde root-end filling, with tooth type identified as the most significant predictor of outcome. PubMed
- A systematic review and meta-analysis confirmed that periapical surgery achieves successful results in approximately 84% of cases overall. MDPI
- When a dental operating microscope and ultrasonic tips are used together, success rates exceed 90% — a significant improvement over traditional techniques. PubMed
- Longer-term data shows some attrition: 77.8% at 2–4 years and 71.8% at 4–6 years, underscoring the importance of proper post-surgical restoration and regular monitoring. ScienceDirect
Microscopic apicoectomy allows for a level of precision that traditional methods simply cannot achieve — and the data reflects that.
Post-Operative Care: What to Expect
Apicoectomy is a minor oral surgery, but patients should be prepared for a realistic recovery period.
Days 1–2: Swelling and bruising around the surgical site are normal. Apply an ice pack intermittently on the day of surgery (20 minutes on, 20 minutes off). Take prescribed analgesics as directed.
Days 3–5: Swelling typically peaks around day 2 and begins to subside. Avoid hard or hot foods. No rinsing or spitting forcefully during this period.
Week 1–2: Suture removal is typically scheduled around day 7–10. Maintain gentle oral hygiene around the site.
Possible complications to be aware of:
- Temporary numbness: In lower molar surgeries, proximity to the inferior alveolar nerve may cause temporary lip or chin numbness. This typically resolves within weeks to months.
- Secondary infection: Rare, but possible. Complete your full antibiotic course.
- Delayed healing: Smokers and patients with diabetes or immunosuppression may experience slower bone regeneration. This should be discussed in your pre-operative consultation.
FAQ
Q. How long does the procedure take? Microscopic apicoectomy on a single-rooted anterior tooth typically takes 60–90 minutes. Multi-rooted posterior teeth may require longer.
Q. Is the procedure painful? The surgery itself is performed under local anesthesia — you will feel pressure, but not pain. Post-operative discomfort is generally manageable with over-the-counter or prescribed analgesics and peaks within the first 24–48 hours.
Q. Can I go back to work the same day? Most patients prefer to take 1–2 days off. Significant swelling and bruising may be visible, particularly in the first 48 hours.
Q. What happens if apicoectomy fails? If the lesion does not heal after apicoectomy, options include re-apicoectomy (in selected cases) or extraction followed by implant placement. The success of a future implant is not compromised by a prior failed apicoectomy.
Q. Is microscope use necessary? Evidence strongly supports the use of a surgical microscope. It is not merely a preference — it directly impacts the ability to detect cracks, verify canal anatomy, and place retrograde filling with precision.
Final Thoughts
In my clinical experience, patients are often surprised to learn that extraction is not inevitable when root canal treatment fails. A well-executed microscopic apicoectomy — using proper incision design, precise root-end resection, and a biocompatible retrofilling material like MTA — can give a tooth a genuine second chance.
That said, outcomes are highly case-dependent. Patient selection, tooth position, bone volume, and restoration quality all play a role. If you’re facing a similar situation, I’d encourage you to seek a consultation with an endodontic specialist before making a final decision.
Preserving your natural tooth is always worth exploring first.